


The Scholar Behind UMS's Master's Program in IQT
27 July 2026
Prof. Andri Nirwana, S.TH., M.Ag., Ph.D., pioneered the Master of Al-Quran and Tafsir Studies as a first step in strengthening Quranic studies within Muhammadiyah.




Every citizen has the basic right to health services. The implementation of the National Health Insurance (JKN) program is a testament to the state’s commitment to safeguarding its citizens. Through JKN, the government steps in to assist the community in shouldering the burden of health costs.
Community health insurance is crucial due to the high costs associated with individual health expenses. The JKN program serves as a “savior” by addressing the challenge of exorbitant healthcare costs for the public.
Countries like Germany, Netherlands, Singapore, and Philippines have successfully implemented the National Health Insurance (JKN) program by adopting a universal healthcare system. This approach ensures that every citizen receives protection and access to affordable healthcare services. Following the lead of other nations with universal healthcare, Indonesia adopted a comparable system through the Social Health Insurance Administration Body (BPJS) on January 1, 2014.
BPJS Kesehatan is crucial in providing convenient, affordable, accessible healthcare. The service is categorized into three classes: class I, class II, and class III. As reported by Bisnis.com, up to September 1, 2023, BPJS Kesehatan has successfully enrolled over 262 million users, encompassing approximately 94.6% of Indonesia's total population.
BPJS Kesehatan, in its execution, follows a pattern distinct from conventional health insurance systems observed in other countries. This observation stems from research conducted by Dr. Arief Budiono, S.H., M.H., a lecturer at the Faculty of Law, Universitas Muhammadiyah Surakarta (UMS). The research, titled “Black Swan Theory: Legal Policy of the Indonesian National Healthcare,” has been published in Legality: Jurnal Ilmiah Hukum.

Arief Budiono provides a compelling depiction of the anomalies within BPJS Kesehatan that distinguish Indonesia’s JKN from those in other countries. Arief as he is familiarly known, based his theory on the black swan to illustrate how the Indonesian JKN program has disrupted various countries' conventional health insurance systems.
Arief Budiono argues that the health insurance system should compel the state to fulfill citizens’ basic rights. He emphasizes that when we mention the JKN program, the state should take part in fulfilling the basic right to health, as mandated by the state constitution.
Regrettably, the term “fulfilled” is not entirely applicable in Indonesia. Instead of the state taking on the responsibility to fulfill health insurance, it is extracting money from the community to fund it. Arief argues that, based on the 1945 Constitution, the state should actively cover its citizens’ health costs.
“In fact, this health insurance is borne by citizens. If you look at the BPJS Law, the state only provides a capital of two trillion. One trillion for BPJS Kesehatan and one trillion for BPJS Ketenagakerjaan. The rest is the state collects levies from its citizens. So where is the presence of the state?” explained Arief.
Not only that, he also outlined the problems that hit BPJS Kesehatan. There are at least six main problems that include:
The principles mentioned in Law No. 24 Year 2011 on Social Security Organizing Agency include nine principles, with gotong royong (mutual cooperation) being the first.
In the pattern of BPJS, the principle of mutual cooperation is reflected in the fact that both healthy and sick citizens contribute by paying premiums. The funds collected are then utilized for the benefit of all members, embodying the concept of gotong royong.
However, Arief's research identified a slight mistake in the application of the mutual cooperation principle. The mistake lies in the parties who remain passive when they should actively engage in seeking mutual cooperation within the JKN program.
Arief points out that while the term gotong royong is correct in the context of BPJS, there is a misplacement of actors involved in mutual cooperation. Currently, the people are actively participating, while the state is not in the same shoes.
Arief emphasizes that the state should actively engage in mutual cooperation with the BPJS Kesehatan member. In this way, mutual cooperation is not solely imposed on the people. Still, it becomes a collaborative effort between the state and its citizens. “The state must be present because it is mandated by the constitution,” he stressed.
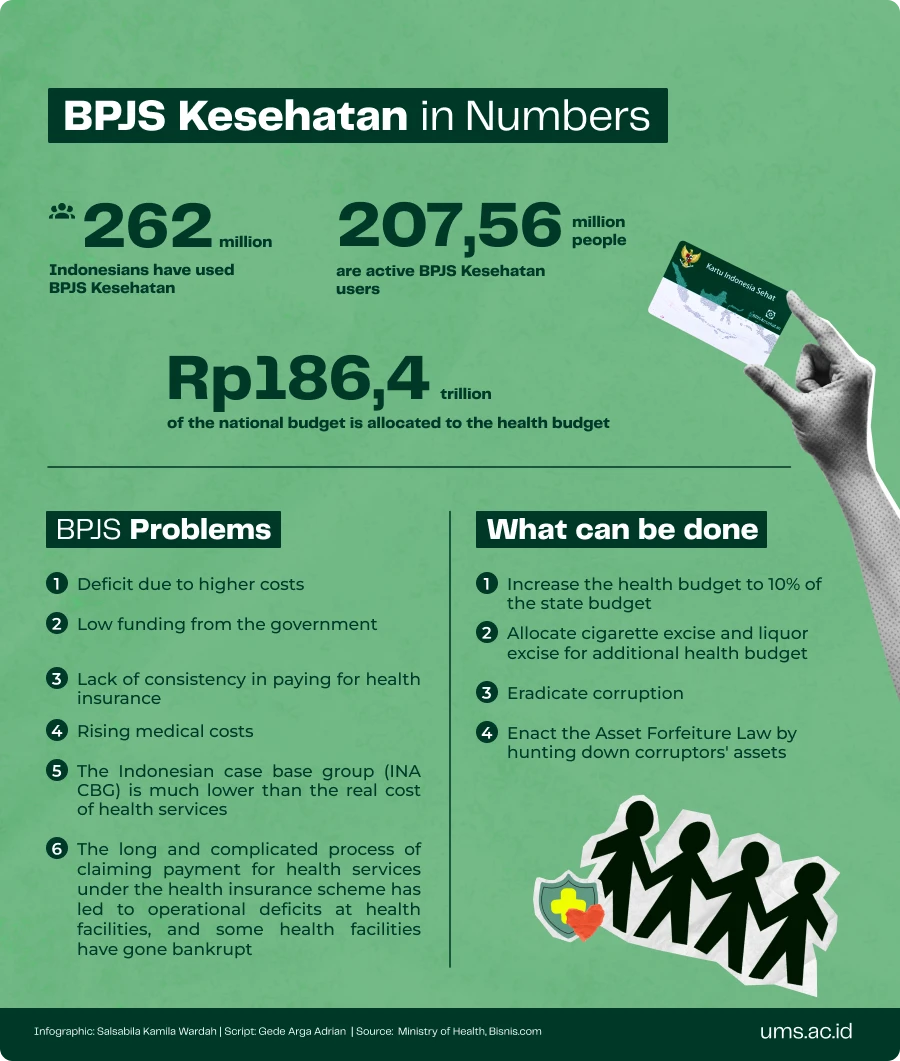
The poisoned chalice of BPJS Kesehatan has exacerbated the challenges of national health insurance. The organization grapples with financial issues, as only 5% of the total budget for health services is allocated from the State Budget (APBN).
“Out of the allocated five percent, only two percent is directed towards BPJS Kesehatan, while the remaining portion is utilized for infrastructure and other medical equipment,” explained Arief.
Apart from budget concerns, Arief highlighted the impact of irregular payments from community contributions on the financial stability of BPJS Kesehatan. The delayed payments from individuals contribute to the cash flow challenges faced by BPJS.
The potential risks associated with non-payment of BPJS contributions should have been considered in Indonesia's health budgeting. Inability to meet contribution obligations can lead to severe consequences, disrupting the JKN services.
“BPJS’ cash flow will automatically turn negative if there are overdue community contributions. When the cash flow is negative, there are two options: go bankrupt or postpone bankruptcy by implementing certain regulations,” he continued.
From various studies reviewed by Arief, it appears that BPJS Kesehatan employs various methods to delay bankruptcy. One commonly used method is to complicate the claim mechanism, leading to significant delays in the payment of hospital claims. This delay poses a challenge for hospitals and health facilities as they have already expended their treatment budgets in advance.
The snowball effect of BPJS Kesehatan’s poor cash flow brings disaster risk to the national health system. Arief did not hesitate to say that hospitals are potentially bankrupt in the current BPJS Health system. This is the result of the BPJS cash balance being stuck.
“Some regulations cause hospitals to wait months to receive health cost reimbursements. This delay in BPJS payments can lead to hospital bankruptcies. On the other hand, hospitals cannot deny patients, including those with BPJS. The hospitals, however require operational funds for various expenses, including building costs, electricity, and employee salaries,” Arief emphasized.
In addition to the risk of bankruptcy, another consequence of the financial difficulties is reflected in the Indonesian-Case Based Groups (INA CBG) costs, which have not increased in recent years. INA CBG represents the claim payment amount made by BPJS Kesehatan to Advanced Referral Health Facilities for service packages based on groupings of disease diagnoses and procedures.
The INA CBG, which has not seen an increase in recent years, is a crucial point to note as it may impact the actual cost of health services. While real costs may increase, the lack of an increase in INA CBG claim costs poses a risk of diminishing health services quality.
“The consequence is that hospitals may reduce service facilities. Failing to do so could pose a problem for the hospital, as the real cost would exceed the BPJS claim. If the claim is lower than the actual cost, it could result in financial losses for the hospital,” he explained.
In countries that implement universal healthcare, the state genuinely participates in fulfilling the health rights of its citizens. A country with a health insurance system similar to Indonesia's is the Philippines. Filipino citizens are required to pay contributions to access health services.
In a universal healthcare system, there is a term called Out of Pocket (OOP), which refers to the amount of money patients have to pay to access health services. The OOP amount can vary depending on the budget allocated by the state.
Arief mentioned that the Philippines allocates a substantial budget for health. This, combined with significant excise taxes on alcohol and cigarettes, has led to a reduction in Out of Pocket (OOP) costs.
“Filipinos are only charged 29-30% Out of Pocket (OOP) fees. This was supported by a sizable budget earlier. This is different from Indonesia, where the OOP fee is in the range of 35-45%. There is a significant difference, so Filipinos can pay less than Indonesians,” he explained.
According to him, the lower the Out of Pocket (OOP), the more people can allocate their personal funds for other needs such as education or savings. “Just add the state budget for health, then OOP will automatically go down,” Arief emphasized.
Arief sees that the state still sees profit and loss in fulfilling the JKN program. This mindset, according to him, must be changed immediately. The state should not see profit and loss in providing the right to health for its citizens. It is time to turn over a new leaf.
According to Arief, there are two strategies that the state can do to increase subsidies to BPJS Kesehatan, namely:
Firstly, additional health funds can be sourced through excise taxes on cigarettes and liquor. It is essential to ensure that the excise tax is not lower than the health costs caused by smoking and alcohol consumption.
Second, the state must be able to suppress corruption. The corrupted budget must be reclaimed to provide additional funds for the JKN program.
“Why not reclaim the funds that were corrupted? That's why the Asset Forfeiture Law must be passed immediately so that the state can confiscate the assets of corruptors,” said Arief.
He hopes that Indonesia’s future leaders should be able to increase the health budget.
“The new leader must have the courage to allocate a health budget. A budget of five percent of the APBN is not ideal. The health budget should ideally be ten percent of the APBN,” he concluded.
Writer: Gede Arga Adrian
Editor: Genis Dwi Gustati
Translator: Farizal Luqman Majid
Prof. Andri Nirwana, S.TH., M.Ag., Ph.D., pioneered the Master of Al-Quran and Tafsir Studies as a first step in strengthening Quranic studies within Muhammadiyah.
A UMS pencak silat athlete successfully claimed gold at the 10th Asian Pencak Silat Championship 2026.

The Klanceng Edufarm startup is planning international expansion after being named national champion at the 2026 Studentpreneur Bootcamp organized by the Muhammadiyah Center for Entrepreneurship and Business Incubator.

Nothing’s more special than reading curated news just for you.
Subscribe to the UMS Newsletter for free today.





